
5.1 Operating Room - What Can We Do to Prevent Injuries?
The musculoskeletal pathology associated with postural problems in the Operating Room (OR) is now a relevant topic for every surgeon.
This chapter aims to identify the potential risks to which an ophthalmological surgeon is exposed, in order to be able to become aware of the posture adopted by each one.
Ergophthalmology hopes to contribute to a preventive attitude towards potential future pathologies, through simple strategies to change posture habits.
It is now known that the ophthalmologist presents a great risk of developing musculoskeletal pathology, and this risk is greater in this area than in other medical specialties.1
Some studies have confirmed this statement:
- Chatterjee A. et al.2 revealed that 54% of ophthalmologists in the UK suffered from lower back pain, presenting more complaints according to the number of years of their clinical practice.2 Nine surgeons required surgical intervention.2
Nove cirurgiões necessitaram mesmo de intervenção cirurgica.2
- Dhimitri KC. et al.3 , in a questionnaire to American ophthalmologists, found that 51.8% had neck and lower back pain in the last month of work, 15% with mild to moderate limitations in clinical practice.3
- A study by Chams H. et al.4 ,revealed that 80% of the participants had lower back pain and about 55% had chronic headache.4
Other occupational pathologies were also more associated with ophthalmologists, such as visual problems related to LASER and the use of the microscope in the OR (15%).4
Visual complaints were more prevalent in vitreoretinal surgeons (p <0.004).4
- Jonathan N. et al.5,observed that 60% of ophthalmologists in the United Kingdom suffered from neck pain or lower back pain, or both.
These numbers were more alarming when they evaluated ophthalmologists in the OR, in which 33.6% reported pain while operating and 78.6% stated that surgery exerted an exacerbating effect of pain complaints.5
For this reason, some ophthalmologists have reduced the hours spent in OR.5
The surgeons most affected by neck pain were, firstly, those of vitreoretinal surgery, followed by oculoplastic and glaucoma surgery, which may be related to the duration of surgery.5
- A study by Al-Juhani M. et al.6 revealed that neck and lower back pain were both presented by younger and older ophthalmologists, revealing that pain symptoms are not only related to the years of clinical practice being a transversal problem to all ophthalmologists.6
- The study by Kitzmann A. et al.7 ,confirmed the higher prevalence of neck and lower back pain in ophthalmologists when compared to family physicians.7
In the OR, during surgery, it is possible to identify several factors that are related with the development of musculoskeletal conditions, which are:
1. Repetitive movements, performed under conditions of stress and cognitive effort, inherent to surgery, which are exacerbating factors of headache and neck pain.5,8
2. Tasks that require very fine control, requiring close vision, which causes muscle tension in the head, neck and upper limbs.8
3. Maintenance of a posture, often inadequate, over a long period (surgery), with the condition of the immobility required in this extreme position.1,8
Although it is not the only specialty that uses the microscope during surgery, in ophthalmology this problem is even more dramatic. In addition to the OR, posture is often inadequate in the clinic (observing patients on the slit lamp) and when doing complementary exams and treatments (LASER).1
When you are using the microscope it is possible to identify several sources of postural problems:
- Head in extension, possible source of spasms and muscular contractures.8
- Arms in suspension, with all static force applied to the shoulders.8
- Holding extremely delicate instruments, which requires the application of a lot of force in fine and precise movements over long periods of time, in conditions of immobility.8
Often too high or too low, with incorrect limb angulation and without support, which causes shoulder pain, carpal tunnel syndrome, and even tendinitis.8
- Poor position of the lower limbs, which seems to exacerbate the surgeon's position and also be a source of discomfort during surgery.8
If we observe the position in which the surgeon is while he is operating, we perceive that the trunk is subject to an intense tension, being the base of support for the simultaneous coordination of the head, that is looking for the microscope, upper limbs, that are holding the instruments, and the lower limbs, which coordinate the microscope and ultrasound pedal, in the case of cataract surgery.9
Data on poor posture presented by most ophthalmologists in the OR show that flexion/extension of the neck in an excess of only 15 ° may be associated with cervical symptoms.5
Due to this static hyperextension on microscope, problems such as degenerative pathology in the vertebral discs and disc hernias are also more frequent in this group of physicians.1,8
All these factors together can provoke severe musculoskeletal pathology that may ultimately be responsible for the need to stop professional activity and even surgical correction.1,8
However, few surgeons can recognize that their posture is incorrect, and do not know the best posture to adopt, in order to avoid posture-related damage in OR.1
Suggestions to correct the posture in the Operating Room:
The surgeon's chair should have a backrest and should be adjusted so that the knees are bent 90 ° with feet resting on the floor / pedals, with the thighs parallel to the floor (Fig. 1).5,9
If necessary, in order to avoid unevenness of the lower limbs, a metal platform may be placed so that a balance is observed in the height of the two limbs.9
Only after the good positioning of the surgeon should the patient's marquise and microscope be adjusted.5,9
The latter and its eyepieces, which must be movable, must be adjusted so that the trunk and neck of the surgeon remain straight, without flexions or extensions (Fig. 2).5,9
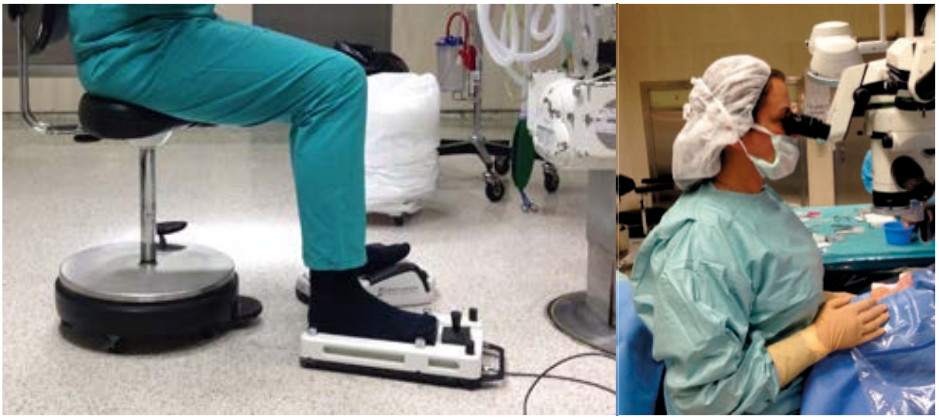
Fig. 1 Correct position of lower limbs. Fig. 2 Correct position of the head and neck.
Often, the taller surgeons are leaning over the microscope, with pain at the level of the neck and possible numbness of the upper limbs.1
The suggestion is to place the cylinder of the microscope up higher, so the surgeon sits with his trunk and neck straight, as if the surgeon is looking at a point, at the level of his eyes, on the opposite wall.
This balance may not be easy if the surgeon and the assistant have very different heights, and the assistant may be in an uncomfortable and potentially harmful position.1,9
Arm rests are generally not advised in surgeries where the patient is awake, because if the arms are "stuck" in one position they cannot easily follow small deviations from the patient's head, making it difficult to see the red eye reflex, such in cataract surgery.1
In surgeries where the patient is under general anesthesia, this may be an option.
In our hospital, for example, the arm support is used in macula surgery, due to the need for a still, maintained and precise position, in which the area that needs to be better visualized is central.
Finally, the surgeon should do physical exercise to compensate for the vicious posture he often adopts, and strengthen the muscles, avoiding excessive muscle tension during surgery.9
The American Academy of Ophthalmology has even launched some exercises, to help muscle relaxation and to prevent musculoskeletal pathology.9
In the future, this problem will be possibly avoided through the new systems of surgery with television viewing, using a system of 3-dimensional glasses.1
In this way, the surgeon will look forward to a monitor placed at the level of his eyes, and there is no risk of being bent over a microscope.1
Nowadays, since the use of a microscope in the OR is our reality, our advice is prevention.
What can we do to prevent injury?
Adopting a correct posture in the OR is the key to avoiding future injuries.
